Gynaecological cancer is one of the most common malignancies affecting women; hence, the need for radical hysterectomy. This disease is usually diagnosed too late, limiting the treatment options, especially in countries like India (due to lack of awareness, shortage of proper screening facilities, and variable pathology).
Going for annual basic full body check-ups along with a gynaecologist consultation can prevent a disease from getting out of a person’s control. Radical hysterectomy is preferred to treat women at an early stage of cervical cancer and has more than 90% cure rate. Although going through radical hysterectomy can cure many ailments including cancer, women will no longer be able to have children post-surgery and have an early menopause.
This post will give you a more than basic understanding of radical hysterectomy, but let’s start with a brief introduction to the female genitalia.
Understanding the female reproductive system
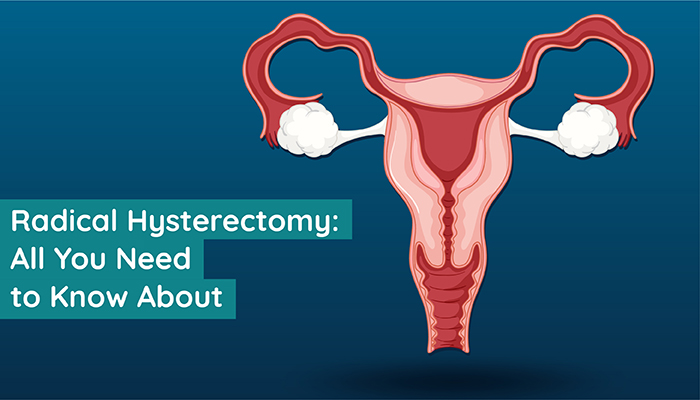
Following is the list of major components of the female reproductive system:- Vagina—a muscular tube attached to the cervix with an opening below the urethral opening (from where you urinate). This tube is where the male sperm is ejaculated during sexual intercourse.
- Cervix—lower part of the uterus (or womb), also known as the neck of the womb, which acts as a gateway for the male sperm to enter the uterus.
- Uterus—an inverted pear-shaped organ between the pelvis where (1) an egg waits for fertilisation and bleeds away during periods along with the inner lining of the uterus or (2) the baby develops after fertilisation.
- Fallopian tubes—tubes that act as passageway to the egg, capturing it from one of the ovaries upon release.
- A pair of ovaries—the storehouses of immature eggs beside the Fallopian tubes, which also secrete female hormones (oestrogen and progesterone). Each ovary releases a mature egg in an alternate month for fertilisation.
What is radical hysterectomy?
Hysterectomy simply means the surgical removal of the uterus. Radical hysterectomy means the surgical removal of the uterus from the root, including the cervix, parametrium (tissues surrounding the cervix and uterus), (sometimes) the upper part of the vagina, both fallopian tubes, both ovaries, and nearby tissues (such as pelvic and abdominal lymph nodes).
This is a procedure used to treat cancer patients with a variety of gynaecological cancers, including ovarian cancer, cervical cancer, and endometrial (inner part of the uterus) cancer. In most cases, a surgeon starts with the objective of removing the uterus and avoiding any unnecessary interference inside the body. The removal of other organs in addition to the uterus depends on what the surgeon finds during the operation.
Although a radical hysterectomy typically does not alter their sexual functioning, it removes the possibility of a woman becoming pregnant. However, for preserving fertility, several alternatives to a radical hysterectomy are available. People are recommended to discuss these alternatives with their gynaecologist and/or oncologist before proceeding with a radical hysterectomy. Treatment plan may differ from woman to woman, and age, medical history, individual diagnosis, financial situation, and personal preferences, all pay a role in deciding the best course of action.
Types of radical hysterectomy
Based on a standard classification (accepted worldwide) presented by Dr. Querlue and Dr. Morrow in 2008 (updated in 2017), there are primarily four types of radical hysterectomy—type A, B, C, and D. The classification was derived by considering three anatomical structures—ureter (carries urine from kidney to bladder), uterine artery (main blood supply for the uterus), and pelvic side wall (ligaments and muscles that line the part of the body between the hips)—as landmarks. Radical hysterectomy classification is achieved by evaluating four levels of surgical plane while decrying the radical extent:- Level of resection (where incisions or cuts are made to divide two organs) of the paracervix (or the connective tissue of the pelvic floor) is taken
- Level at which bladder and rectal pillow are taken
- Vaginal margin taken
- Overall goal of the procedure
- Type A radical hysterectomy
- Type B radical hysterectomy
Type B has two subtypes, B1 and B2. The major difference between these two is that in Type B1, lateral paracervical lymph nodes are not removed, and in Type B2, they are removed.
- Type C radical hysterectomy
Type C also has two subtypes; in Type C1, the autonomic nerves (a part of the involuntary physiological functions of the body) are preserved, and in type C2, they are not preserved.
- Type D radical hysterectomy
One may notice that as these procedures progress from Type A to Type D2, the number of organs removed also increases.
There are 3 common approaches used by doctors for performing radical hysterectomy:
- Laparoscopic or keyhole surgery
- Abdominal hysterectomy
This approach may be recommended if the womb is enlarged by fibroids (a benign tumour) or pelvic tumours that make it impossible to carry out the procedure through the vagina. In addition, if the ovaries are required to be removed, the doctor may ditch the vaginal hysterectomy.
- Vaginal hysterectomy
- General anaesthesia, which renders the patient unconscious
- Local anaesthesia, which numbs the area so that the patient does not feel any pain
- Spinal anaesthesia, where the body goes numb from the waist down
- Robotic surgery
The surgeon controls the movements of a set of equipment’s attached to a robotic arm with high precision with the help of a video camera for guidance.
Need for radical hysterectomy
A well-known procedure for treating gynaecological cancer in oncology, radical hysterectomy is recommended only when other forms of treatment (including chemotherapy) either don’t work or cannot be administered to a patient. However, cancer is not the only reason why the gynaecologist might recommend a radical hysterectomy. Here’s a list of common reasons for a radical hysterectomy:- Heavy periods (which may be caused by fibroids)
In some cases, radical hysterectomy (removing the uterus) may be the only viable option when other treatment options don’t work or the woman chooses to have a surgical menopause (more on this later) after careful consideration.
- Pelvic inflammatory disease (PID)
A radical hysterectomy is proposed as the only option when the infection is too large to be treated by just medicine and the woman is prepared for a surgical menopause.
- Endometriosis and adenomyosis
If other treatment options do not show any signs of improvement, a radical hysterectomy may be recommended during a follow-up gynaecologist consultation as the last resort.
- Fibroids
A radical hysterectomy may be performed if a woman has large fibroids or severe symptoms.
- Adenomyosis
- Prolapse of the uterus
Childbirth can often lead to a prolapsed uterus, and radical hysterectomy removes the entire uterus.
- Cancer
Apart from cancer, one should reflect on the following questions and discuss them with their doctor, during the gynaecologist consultation, when thinking about having a radical hysterectomy:
- Are my symptoms severe and hindering my day-to-day functions?
- Are there no alternative treatments for my condition?
- Do I want children?
- Am I ready to have an early menopause?
Getting ready for a radical hysterectomy
Once the decision is made, you should start preparing the body for the procedure. Being in a healthy physical state can reduce the chances of any risks of complication and speed up the recovery process. One should do the following to prepare their body for this surgery:- Stop smoking
- Eat a balanced diet
- Exercise regularly and try to attain a healthy weight
Before the surgery the doctor or a nurse will give you a briefing about instructions related to anaesthesia. If the doctor decides to go with general anaesthesia, you might have to stop eating at least 6 hours before the surgery and stop drinking water 2 hours before the procedure. Your vital signs will be checked right before the surgery to make sure you are ready for it.
Risks and side effects involved with radical hysterectomy
As with any other surgery, a radical hysterectomy carries its own set of risks and complications. Here’s a list of complications:- Deep vein thrombosis (blood clots in legs) or pulmonary embolism (blood clots in lungs) usually occurs within first 5 weeks of surgery and can be cured in some time
- Severe bleeding or haemorrhages during the surgery, which requires blood transfusion
- Allergic reaction to anaesthesia, which may require the surgeon to manage the reaction first to avoid any life-threatening situation and the surgery (if it is an emergency procedure) will be continued only after the patient vitals are stable
- Injury to other internal organs such as ureter, bladder, or bowel
- Infection (with symptoms like high fever), which may require medical attention
- Vaginal problems (after a vaginal hysterectomy) can range from slow recovery or infection to prolapse in advanced age
- Pain while having sex
- Failure of ovaries leading to symptoms of early menopause including hot flushes, vaginal dryness, disturbed sleep, and excessive sweating
Recovery after radical hysterectomy
Usually, a woman stays under observation at the hospital for anywhere between 1 and 3 days, and it may take about a month or so post-hospitalisation to completely recover from the surgery. Regular gynaecologist consultations should be planned in advance to check the recovery. During these consultations, the doctor will share precautions accordingly and may also advice regular basic full body check-ups at least for a few months post-surgery.
If the cervix is not removed during the surgery for any reason, you will need to go for regular cervical screening tests along to ensure it stays healthy. You can discuss any discomfort or a troubling symptom in the follow-up consultations. The removed organs also go for biopsy to check for conditions like cancer, endometrial hyperplasia, among others. The results of this test may be relayed to you during follow-up appointments or over the phone.
Some women may be recommended hormone replacement therapy (HRT) to help with the symptoms of an early menopause if both their ovaries are removed. The procedure is meant to supplement the lack of necessary hormones secreted by ovaries. However, women who have had a hormone-dependent breast cancer or a liver disease cannot opt for this treatment. Women for whom HRT seems to work may have to continue regular treatment till the average age of natural menopause, which is around 51.
Reclaiming the normal life after radical hysterectomy
This will vary from person to person as the recovery rate is different for everyone.- Returning to work
- Driving
- Workout and weight lifting
Make sure you do not lift heavy weights until the doctor gives a green signal as it may cause severe damage to your internal organs; always ask someone for help. Even while lifting lightweight objects make sure to bend your knees slightly and keep a straight back, but avoid lifting any weights whenever possible.
- Sex
Many women experience a temporary loss of sexual desire (libido) after the surgery. Some experience vaginal dryness if ovaries are removed and they are not taking HRT. However, having sex should not be a problem as long as you are comfortable.
- Contraception
Final word
Whether you have cancer or going through radical hysterectomy for a different reason, make sure you follow the doctor’s guidelines for a speedy recovery after the surgery. Booking gynaecologist consultations for an annual visit (at the least) is a good practice to ensure that no complications are developed over time.
Surgical menopause can be overwhelming for some women; thus, it is always advisable to talk to the doctor about any concerns (big or small) related to radical hysterectomy.
