
What Is a Neurofibroma?
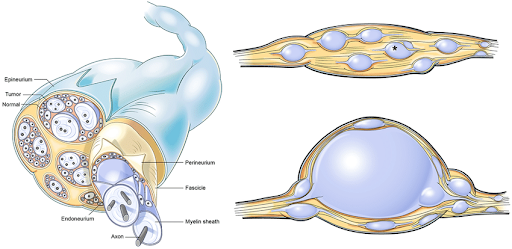
“Neurofibroma meaning”; this term means a benign nerve-sheath tumor that develops along peripheral nerves. These growths are sometimes described as a soft bump under or on the skin. They happen because of an overgrowth of several cell types within the nerve sheath.
Although a neurofibroma tumor is usually not cancerous, it may become problematic depending on size or location. Some people develop a single growth called a solitary neurofibroma, while others have multiple lesions. This is especially the case when linked with a condition known as neurofibromatosis type 1.
What are the types of neurofibromas?
The range of neurofibroma types is broad, differentiated in depth, location, and behavior. Understanding these types helps clarify why treatment or symptoms vary. Some key categories include:
- Dermal neurofibroma: These occur on or just under the skin’s surface. They often appear as soft, skin-coloured papules or nodules.
- Solitary neurofibroma: A single isolated lesion in someone without NF1. It might not be associated with a larger Genetic Syndrome.
- Plexiform neurofibroma: A more complex growth involving multiple nerve bundles or plexuses; the term plexiform neurofibroma itself refers to this tree-like, sprawling pattern.
- Spinal neurofibroma: When the growth occurs along nerves exiting the spine, it may press on spinal structures and cause specific neurological symptoms.
- Myxoid neurofibroma: A rarer subtype where the histological background shows a myxoid matrix (a jelly-like extracellular component) — when you read about neurofibroma histology, this term may appear.
- Neurofibroma type 1 (NF1-associated lesions): In the context of NF1, multiple neurofibromas (including plexiform and dermal types) may occur along with other signs.
In short, whether you’re dealing with a dermal nodule or a deeper plexiform mass, recognizing the type helps tailor management and expectation of outcomes.
What are the Neurofibroma Symptoms?
Symptoms depend largely on the location, size, and type of the neurofibroma. A small dermal neurofibroma skin lesion may cause minimal concern, while a deep plexiform or spinal neurofibroma can cause more significant issues. Typical symptoms include:
- A visible bump or lump on the skin surface — often skin-coloured or slightly darker — is seen in dermal or cutaneous lesions.
- Tenderness, pain, or itching where the tumor is located (especially if it lies under or near the skin surface).
- Sensory changes like tingling, numbness, or weakness when the growth compresses a nerve (more common in spinal neurofibroma or deep lesions).
- Cosmetic or functional issues: For example, a large plexiform neurofibroma may lead to disfigurement of limb or facial structures; a spinal neurofibroma may interfere with mobility or cause gait problems.
Overall, many neurofibromas remain asymptomatic for years, especially if small and superficial. Because symptoms vary widely, recognizing the possibility of a neurofibroma tumor and seeking evaluation when changes occur (growth, pain, functional impairment) is important.
What are the Neurofibroma Causes?
When considering neurofibroma causes, it’s useful to recognize both sporadic and inherited pathways. For many people, a solitary neurofibroma arises without a clear inherited disorder. But in the case of neurofibroma type 1, the underlying cause is a genetic mutation in the NF1 gene, which encodes neurofibromin, a tumor-suppressor protein. Loss of function of neurofibromin promotes unregulated growth of cells in the nerve sheath.
Additional details around causes:
- The mutation in NF1 often follows an autosomal-dominant inheritance, though many cases are new (de novo).
- For a plexiform neurofibroma, especially in NF1, the risk is higher, and these lesions often develop early in life.
- Although the exact mechanism for solitary lesions is less clear, they still share histologic features (as seen in neurofibroma histology) such as a myxoid matrix and spindle cells.
Other possible contributing factors include local trauma or irritation (although this is less clearly proven) in sporadic cases. Understanding the cause helps guide monitoring and alerts both patients and providers to potential progression (especially in NF1-associated cases).
How do doctors diagnose this condition?
Diagnosing a neurofibroma tumor typically involves a combination of clinical examination, imaging, and sometimes biopsy. Here are the standard approaches:
- Clinical & skin exam: For dermal or cutaneous lesions (dermal neurofibroma skin bumps), the physician inspects size, number, location, and any associated signs of NF1.
- Imaging studies: For deeper lesions (such as a spinal neurofibroma or significant plexiform neurofibroma), MRI or CT scans help determine size, nerve involvement, and relation to surrounding structures.
- Histology / biopsy: The phrase “neurofibroma histology” reflects the tissue characteristics seen in pathology. For example, myxoid matrix, spindle cells, collagen bundles, and mast cells.
- Genetic testing/family history: In suspected cases of NF1 (i.e., neurofibroma type 1), genetic evaluation may be advised. Also, monitoring of café-au-lait spots, freckling in the axilla/inguinal region, and other features helps.
Accurate diagnosis ensures the right path for neurofibroma treatment and monitoring.
How is neurofibroma treated?
Choosing a method of neurofibroma treatment depends on the type, location, size, symptoms, and risk factors. Here’s a breakdown of the main strategies:
- Observation: Many superficial dermal neurofibromas cause no pain or functional impairment, so periodic monitoring is often appropriate.
- Surgical removal: When the tumor causes pain, functional impairment. For instance, a spinal neurofibroma causing nerve compression, or one that is disfiguring (especially in plexiform neurofibroma), surgical excision is standard.
- Laser or dermatologic techniques: For dermal neurofibroma skin lesions, especially in NF1, techniques such as CO2 laser ablation are sometimes used for cosmetic or symptomatic relief.
- Targeted drug therapies: Particularly for inoperable plexiform neurofibroma (PN), newer therapies (such as MEK inhibitors) are being used or studied.
- Supportive care: Pain management, physical therapy (especially for spinal neurofibroma), monitoring for malignant transformation, and managing associated NF1-related complications.
When considering plexiform neurofibroma treatment, the complexity is higher because the lesions often involve large nerve bundles and infiltrate surrounding tissue, making full excision difficult. In essence, the goal of treatment is to balance symptom control, functional preservation, and quality of life.
When should I see the healthcare provider?
You should consult a healthcare provider if you notice any of the following:
- A new bump on the skin or under it that is growing, changing in appearance, becoming painful or tender (possible dermal neurofibroma skin lesion).
- Persistent pain, numbness, tingling, or weakness in a limb or area suggestive of a deeper growth, like a spinal neurofibroma.
- Enlarging or disfiguring lesions that are affecting your appearance or function (especially in a known case of neurofibroma type 1 or other syndrome).
- Symptoms such as rapid growth, changing texture, sudden onset of pain, or neurological symptoms (may hint at malignant transformation).
- For individuals with NF1, regular monitoring is critical because of the risk of new lesions and complications linked to plexiform neurofibroma.
Don’t ignore any new or changing growths, talk to a neurologist online for accurate diagnosis and timely care to prevent possible nerve or tissue complications.
Complications of Neurofibroma
While many neurofibromas are benign and relatively harmless, there are potential complications that make awareness important:
- Nerve compression: Especially with deeper or spinal lesions (e.g., spinal neurofibroma), compression can cause pain, numbness, muscle weakness, or functional impairment
- Disfigurement or cosmetic burden: Large or numerous dermal or plexiform lesions can impact appearance, self-esteem, and quality of life
- Malignant transformation: In particular, plexiform neurofibroma associated with NF1 carries a small but real risk of turning into a malignant peripheral nerve-sheath tumor
- Functional loss or organ involvement: If the tumor presses on vital structures (e.g., airway, spinal cord, blood vessels), significant complications can arise
- Associated syndrome risks: For example, people may also face bone deformities, learning disabilities, and vascular issues. So, a lesion labeled as a “neurofibroma tumor” is part of a broader spectrum of challenges.
Due to these potential complications, appropriate monitoring and timely neurofibroma treatment are key.
Key Take aways
- Neurofibroma meaning: It is a benign tumor arising from the peripheral nerve sheaths; it may appear superficially or deeply.
- Some tumors are solitary neurofibromas, but many occur in the setting of neurofibroma type 1 (NF1), a genetic condition.
- There are multiple categories, such as dermal neurofibroma skin bumps, spinal neurofibroma pressing on nerves, and more complex growths like plexiform neurofibroma or myxoid neurofibroma.
- Recognizing the neurofibroma vs schwannoma difference is helpful: Neurofibromas are mixed cell-type tumors with characteristic features, while schwannomas originate from Schwann cells with distinct histology.
- Symptoms vary from minimal to severe, largely depending on size, type, and location.
- Diagnosis involves clinical assessment, imaging, and sometimes biopsy.
- Neurofibroma treatment ranges from observation to surgical removal, laser ablation, and, in complex cases, newer drug therapies.
- Seeing your provider early for changes in a lesion, new neurological symptoms, or changes in known lesions is advisable.
- Complications include nerve compression, cosmetic issues, risk of malignancy (especially with plexiform types), and broader issues in NF1, so regular follow-up is important.

